Antenatal Care
Promoting good physical and mental health throughout the pregnancy and to make sure that all is well with the mother and baby.
Promoting good physical and mental health throughout the pregnancy and to make sure that all is well with the mother and baby.
The purpose of antenatal care is to promote good physical and mental health throughout the pregnancy and to make sure that all is well with the mother and her baby. It also aims to identify problems early and to treat them appropriately.
Having regular check-ups is important for you and your baby.Your return visits during the pregnancy will be shorter than the first visit and it is very important to attend them.
You may have your haemoglobin (iron level) rechecked. This is a blood test. If you are rhesus negative, you will already have received information in the post about your blood group and depending on your baby’s blood group you will be offered an injection of Anti-D. It may be necessary to do other specialist blood tests at this stage of the pregnancy, for example, if you develop high blood pressure or a body itch. Always talk to your midwife or doctor if you have any worries. They will be able to advise you and keep you informed of your progress.
If your due date arrives and you have not gone into labour, your pregnancy is now termed ‘post mature’ or simply, overdue. Nearly half of all pregnant women are still pregnant at 40 weeks but most will go into labour in the coming week. You will be seen again in the antenatal clinic at 41 weeks if you still haven’t gone into labour.
The doctor will discuss your care plan with you. If by any chance you can’t make it to an antenatal appointment, please email your clinic so that another appointment can be scheduled.
Towards the end of the pregnancy, your appointments will be more frequent. In the last few weeks, your GP, midwife or hospital doctor will probably see you on a weekly basis.
Pregnancy is one of the most important journeys that you will ever go on.
To help you understand as much as possible about your pregnancy, this section will take you through your pregnancy week by week, to the day of the birth of your baby and it will give you information on the things that you should do during the different stages of pregnancy.
Generally, you will start feeling the baby move between 18 – 22 weeks. In the beginning, the movements are very gentle and will become stronger as the baby grows. Towards the end of pregnancy, many people will say the baby will stop moving as it runs out of space. You should be able to feel your baby kick every day right up to the day of birth.
Every baby’s movements are different and it is very important that you are aware of your own baby’s pattern of movements. If, in the late stages of pregnancy, you are feeling less movements than normal or a change in movement pattern, you should come into the hospital, as the baby may require further monitoring. Please phone the assessment and emergency unit for advice if needed – 01 817 1700
Most people talk about pregnancy lasting for nine months, but we generally measure pregnancy by weeks, lasting 40 – 42 weeks from conception. Your doctor or midwife will calculate the date you can expect your baby to be born based on the first day of your last menstrual period. They base it on you having a regular cycle of 28 days.
To calculate your expected date of delivery (EDD) add seven days and nine months to the first day of your last menstrual period. For example, if the first day of your last period was on the 2nd of March, your expected date of delivery (EDD) is the 9th of December. Most women will go into spontaneous labour between 37 – 42 weeks of pregnancy. There is no way to accurately predict the exact delivery date.
Medically a pregnancy is divided into three trimesters. The first trimester (12 weeks) is the crucial period when all the organs, muscles and bones of your baby are formed. The second trimester is taken up with rapid growth of your baby. During this time you will start to feel your baby kicking; your baby will be able to swallow and make facial expressions and can hear sounds. In the third trimester, from 28 weeks the baby will undergo an important final phase of growth and maturation of all its organs in preparation for birth.
Week 0-12
During the first trimester your baby will grow from a cluster of cells into a recognisable fetus (baby) that is 5 cm (2 inches) long. It is the time when the foundations of your pregnancy are being laid down. The tiny cells produce hormones that will send signals to your body to stop your periods. The different layers of the cells will develop to create specific parts of the baby’s body. By week five the building blocks for your baby’s organs are already in place. The heart begins to form and circulate blood. The position of the spine and digestive system are in place. Your baby is only 2 mm long at the end of week 5.
Your changing body
In the first few weeks of pregnancy you will not look or feel pregnant, yet your body is already having major changes because you start to produce a lot of pregnancy hormones immediately after conception. The hormone oestrogen thickens the lining of your womb (uterus) and other hormones help the baby to settle down in your womb. Some women are very sensitive to the changes in their body and they know they are pregnant even before they miss a period. Women often feel that their breasts are more tender; you may notice that you want to pass urine more often, and for some women they can feel tired and sick.

Things to do:
Weeks 6-10
During these four weeks, your developing baby will start to change a lot in appearance, so by week 10 your little baby is starting to look like a human being. At week 6 your baby is sprouting limb buds from which the arms and legs will develop. The head continues to grow quicker than any other part of the body in order to accommodate the developing brain. By the end of week 6 your baby is 5 mm (0.2 inch) long.
Week 7
Your baby is 12 mm (0.5 inch) long and the heartbeat can be seen on ultrasound scan. Your baby’s eyes and ears are developing quickly; by the end of week 8, the eyes already contain some colour. Your baby is now 15 mm (0.6 inch) long.
Week 9 – 10
The folds of skin making up the limb buds start to form cartilage, which will later grow into bones. You can see your baby’s movements on ultrasound but you will not feel any of this for some time. The baby is 22 mm (0.9 inch) long by the end of the week 10. You can recognise its eyes but they will stay hidden behind sealed lids and cannot work until later in the second trimester, when the nervous system forms. The heart has developed with four definitive chambers; the heart is beating 160 times per minute. Your baby is now 33 mm (1.3 inches) long.

Week 11
Your baby’s face is fully formed; the liver, stomach and spleen are all in place. You can see the baby’s ears, and the inner ear, which is responsible for balance and hearing, is formed. Your baby has 32 permanent teeth buds. The baby is now 40 mm (1.6 inches) long.
Week 12
Your baby now looks like a human being; its spine, fingers and toes are fully formed. Your baby is now 5 cm (2 inches) long and weighs 18 grams (0.6 ounce). It is during this initial period of development that things like drugs, viruses and environmental factors (anything that comes into direct contact with the mother or baby) can easily damage a baby; so pregnant women should avoid all of these.
Your changing body:
During the early stages of your pregnancy your uterus (womb) will grow a lot in size. By eight weeks it is the size of a medium sized orange, while at 10 weeks it is the size of a grapefruit. To make your womb grow, blood flow from your heart increases. Because of these changes in your circulatory system, you will become aware of differences in the way your body is working; for example changes in your breasts, wanting to pass urine more often and your skin will either become clearer or drier than usual.
Physically some women go through the first trimester feeling well, however, it is common to feel very tired, and nausea can be a major problem. Morning sickness is the most talked about side effect of pregnancy, as 70 – 80% of women will experience it. Morning sickness can happen at any time of the day. Occasionally, some women cannot keep any food or drinks in their stomach and they become dehydrated and weak. If you have severe vomiting, feel dehydrated or weak or are unable to tolerate food or fluids, please attend the emergency room.
Emotionally, you may find your moods change a lot. One minute you could be talking excitedly about the pregnancy and the next you are crying over something very unimportant. This is because of the major hormonal changes that happen in early pregnancy and will settle later in your pregnancy.
In the second trimester, your baby will grow steadily and the baby’s organs will develop more. The overall size of the baby will increase by four times and its weight will increase by 30 times.
By week 13:
Your baby’s facial bones are complete and the delicate facial features are more easily recognised. The head is the largest part of the baby but very soon its body growth will catch up. Your baby at this time is very thin and is covered by a fine translucent skin. Although the eyelids are fully formed, they will stay closed for the most part of the second trimester. Your baby can be seen moving freely on ultrasound scan. The placenta (afterbirth) is formed, which provides oxygen and nutrition from your circulation to the baby. Your baby by the end of week 13 is 6 cm (2.4 inches) long and weighs about 30 grams (1 ounce).
Week 14:
Your baby can make a fist and suck its thumb. Your baby’s arms are long enough for its hands to meet together over its body. The amniotic fluid or liquor (sac of water around the baby) is increasing which is important so that your baby is freer to move which helps the baby’s muscles to develop. Your baby’s kidneys start to work. By the end of this week your baby has grown to 7 cm (2.7 inches) and its weight has gone up to 45 grams (1.5 ounces). Over the next few weeks, your baby grows at a regular rate; its legs in particular have an amazing growth spurt and are now longer than the arms. From now on, your baby’s rate of growth of its body and limbs will slow down; however, your baby will continue to put on weight at a steady pace. This physical slow down helps your baby to develop in different ways. For example, its lungs, digestive and nervous systems are slowly maturing.
By the end of week 16:
Your baby will measure 9 cm (3.5 inches) and weigh 90 grams (3 ounces).
Week 18:
It is possible that you are now feeling your baby kick for the first time. In the beginning you may think it is ‘wind’ until you realise there is a pattern to these gentle movements. Your baby at this stage can know the difference between sweet and bitter flavours as its taste buds are developed. Your baby can open its mouth and stick out its tongue, which you can often see on ultrasound. A very fine hair called lanugo covers the baby’s entire body; it is thought that this helps to keep the baby warm until it has enough fat stores.
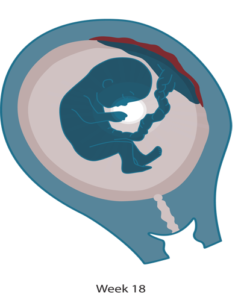
Your baby’s teeth are formed in its gums. Your baby can hear sounds from outside your body and will respond if you play loud or easy music. All these developments in your baby’s senses are due to the fact that its nervous system is developing and maturing.
By the end of the 20th week:
Your baby measures 13 cm (5 inches) and weighs 240 grams (8 ounces). Most women are aware of their baby’s movements around this time.
By 24 weeks:
Your baby is 17 cm (6.5 inches) long and weighs about 500 grams (17.5 ounces). Your baby is able to open and close its mouth and can swallow a large amount of amniotic fluid.
By the 26 week:
The volume of amniotic fluid has increased to about 500 mls. Even though your baby’s lungs are not quite fully developed, the baby has now reached a level of development where it may survive outside the womb with the help of specialist care in the neonatal unit.
In the weeks leading up to week 28:
Important developments are happening inside your baby’s body. Because your baby’s nervous system and skeleton are developing more, the baby’s movements become more deliberate. Your baby can move freely, somersault and hiccough. It is even thought that the baby can tell the difference between you and your partner’s voice. You will also notice a pattern between your baby being asleep and awake; however, this often does not match your own every day and night pattern.

Your changing body:
Now that you are in the second trimester of your pregnancy, you will be much more confident that your baby is a reality. You will probably feel less sick and start to get more energy back into your life. You will also notice that your waist is beginning to get bigger and a bump is beginning to form in your tummy. You can get increased pigmentation of your skin at this time and as a result you will notice the area around your nipples (areola) will become darker. Also, a dark line may form down the centre of your tummy, which is called linea nigra, and moles and birthmarks will also get darker. All these changes are very normal and happen because you have more of the hormone oestrogen in your body.
There is a huge increase in how much blood goes around your body. For example, at the beginning of the second trimester 25% of your blood is directed to your womb in order to support your growing baby and placenta (afterbirth). Just 2% of your blood volume went to your womb before the pregnancy. Because of this some women will feel their heart beating faster and may complain of having palpitations.
As your womb continues to grow you may notice that you develop stretch marks on your tummy and/or around your breasts. This is caused by the collagen beneath the skin tearing as it stretches, as your body gets bigger. There are a number of lotions and creams that you can buy, which may help to reduce the effects of the stretch marks. You will also find that you will feel hungrier as you start to enjoy your meals again. It is important that you eat a balanced diet and remember that it is the quality of the food rather than how much you eat that counts.
![]()
Things to do:
Weeks 28-42
Early in this trimester your baby is able to survive if delivered, although it would still need medical help and constant monitoring in the neonatal unit. The last weeks in the womb are very important as it helps the baby’s lungs, digestive system and brain to develop further in order that they can work well when your baby is born.
Week 29
Your baby will weigh about 1 kg (2.2 lbs). From now until week 32 your baby can put on as much as 500 grams (17 ounces) in weight a week. Your baby’s lungs will be producing a substance called surfactant, which the baby needs to help it breathe after birth, by helping its lungs to be as elastic as possible to be able to expand fully. You will find that your baby’s movements are much stronger and you recognise a definite pattern of movements. Your baby’s eyes are opening and closing and he or she is learning to focus. Your baby’s fingernails reach to the tips of its fingers but its toenails will still need a few more weeks to reach the end of the toes.
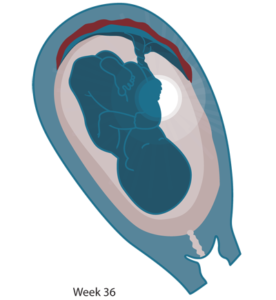
Most babies will lie head down (cephalic) by week 34 especially if it is your first baby. However, some babies will take another week or two before they will settle down in position for birth. Indeed some babies will decide to come bottom first (breech). If by 37 – 38 weeks your baby is not in the cephalic (head down) position, the doctor and midwife will talk to you about birth options. By 36 weeks your baby will weigh 3 kg (6.5 lbs) and you are now in the final lap before birth.
From week 36:
Your baby’s organs are being fine-tuned for birth; the lungs mature, and the digestive system can take liquid foods. The lanugo hair will start to disappear from your baby’s body and his or her immune system can give protection against a variety of infections. If your due date arrives and you have not gone into labour, don’t worry as this is very common, especially for first time mothers.


Your changing body:
Your womb is getting bigger at a steady rate and your stomach and intestines get squashed which means you can get heartburn. Your bladder is also not used to this pressure and can no longer hold as much urine, so you may want to go to the toilet more often. Sometimes you might get a small leak of urine when you sneeze, cough or laugh; this is called stress incontinence. Some women are not sure if the baby’s waters are broken. If you are not sure you should check with your midwife or doctor. Many women will complain that they feel breathless, because their womb is growing and it pushes the contents of their tummy up against their diaphragm so their lungs have less room to expand when they try to take a deep breath.
Your body needs to hold extra fluid and this generally settles on your legs and hands; because of this you will notice they may become swollen. However, if your face or legs suddenly become puffy or swollen it could be a sign of pre-eclampsia and you should go to your doctor or midwife as soon as possible.
With your growing womb you may have problems with sleeping and doing every day things such as shopping or cleaning. Lack of sleep can affect how you feel physically during the day. Lying on your back can be difficult as it can lower your blood pressure and make you feel light-headed. It is best if you can lie on your side with the support of a pillow at your back.
From now until the end of your pregnancy, your womb will start to practice contracting so it can prepare for labour. These tightenings are called Braxton Hicks contractions. In the beginning these can be very mild; however, near the end of the pregnancy they can become strong and uncomfortable. Emotionally, you may find it hard to concentrate on specific tasks; you can become weepy for no particular reason.
Things to do:
We provide diagnostic scans, blood and other screening tests to out rule possible abnormalities with your baby. The staff working in this area are highly specialised and will provide you with all the support and advice you may require.
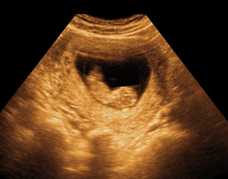
Women are offered an ultrasound scan at their booking visit. This scan is able to check your dates, the number of babies you are expecting and it will show you the baby’s heart beating. You will need to have a full bladder for any scan before 15 weeks.
Fetal Anatomy Scan
All women attending the Rotunda Hospital are offered a detailed ultrasound scan at about 20-22 weeks to see if their baby is developing normally. This is known as the fetal anatomy scan. A large amount of detail about your baby will be visible at this scan. Seeing your baby on the ultrasound screen is a very exciting and emotional time.
What can this scan detect?
This ultrasound scan is very accurate but it cannot diagnose all birth defects. Sometimes, we cannot get clear images of the baby due to the way that your baby may be lying in the womb or because of the mother’s size. If the scan is complete, we would expect to pick up at least:
This scan can also identify 50% of babies with Down syndrome, but the first trimester screening (FTS) test and non-invasive prenatal test (NIPT) are better for this. Because 30-50% of babies with Down syndrome appear normal on ultrasound, only a chorionic villus sampling procedure or amniocentesis can give you this information for certain. It is also important to realise that ultrasound scans in pregnancy do not detect problems like cerebral palsy or autism.
While some babies with chromosomal abnormalities have these soft markers, it is important to remember that 15% of normal babies have at least one ultrasound soft marker. The only way to diagnose or exclude a chromosomal problem for certain is to have an amniocentesis. If you would prefer not to know about these markers please inform us prior to the scan.
If the scan suggests a problem or an abnormality, you and your partner will be informed. We will arrange for you to meet with a consultant who specialises in fetal medicine as soon as possible or within 2 working days.
A full support service will be available for you should any problems be detected, including referral to appropriate specialists. It is important to remember that you will be involved in all decisions regarding the management of your pregnancy. A copy of your report will be sent to your referring hospital, doctor or midwife to ensure good communication.
Why have a fetal anatomy scan?
The vast majority of babies are normal. However all women, whatever their age, have a small chance of delivering a baby with a physical or mental disorder. Many such abnormalities can be diagnosed or ruled out with the fetal anatomy scan.
Reasons to have this scan include:
When you attend for this scan we will tell you about everything that we see, unless you advise us that there are certain things that you don’t want to know about, such as the sex of your baby or markers for chromosome problems. Should you have any questions or concerns please contact the staff in the prenatal diagnosis clinic by phoning 01 872 6572.
Scans in Late Pregnancy
The anatomy scan is usually the last scan taken during pregnancy unless you are referred by the medical team for further scans. Ultrasound scans can also be used in late pregnancy to determine if the baby is growing properly and to check the liquor or fluid around your baby. They help to compile a ‘biophysical profile’ of your baby. This profile is a list of things that are checked and given scores by the midwife or doctor to see how well your baby is doing. The things checked and scored include the baby’s heart rate, the baby’s muscle tone, breathing movements and the amount of fluid around the baby. Other reasons for ultrasound scans in late pregnancy are if there is a possibility your waters have broken or to locate the exact position of the placenta. However, towards the end of pregnancy it can be difficult to get a complete picture on the printout, as the baby is now too big.
Fetal medicine focuses on the management of high risk pregnancies and includes the assessment of fetal (unborn baby) growth and the diagnosis of fetal illness and abnormality. Fetal medicine can be broadly divided into two branches: prenatal diagnosis and fetal treatment. Prenatal diagnosis is the ability to detect abnormal conditions of the fetus. The most common test used for prenatal diagnosis is ultrasound. Some abnormalities may be identified from additional blood screening or invasive diagnostic tests. Fetal treatment includes a series of interventions performed on the fetus with the aim of achieving fetal wellbeing. These interventions include medical (non-invasive) and surgical procedures.
Contact details:
Phone: 01 – 872 6572
Email: [email protected]
Referral form:
Fetal Medicine Referral Form.docx
Please complete the form if you wish to refer a woman to the unit for review or treatment.
Prenatal Diagnosis Clinic
The prenatal diagnosis clinic (PNDC) provides pregnancy screening, diagnostic testing, intrauterine therapies, and patient support and counselling. We provide a standard of excellence in the field of prenatal diagnosis and fetal medicine for patients from our own catchment area as well as for women referred to the clinic from other centres around the country. Our ultrasound scans are performed to the highest international standards and women are supported by informative and sensitive counselling services. Women and their partners receive personalised care by a team of specialist doctors and midwives.
Services Provided Include:
Non-invasive prenatal testing (NIPT) is a screening test that helps to identify if your baby is likely to have a chromosomal condition, for example, Down syndrome (Trisomy 21), Edward syndrome (Trisomy 18) or Patau syndrome (Trisomy 13). The blood test can be performed from 10 weeks of pregnancy onwards. There is no risk of miscarriage associated with this screening test. The test can be helpful in deciding if an invasive screening test is required to out rule one of the syndromes mentioned above.
This test is not carried out routinely on all pregnant women. It is an ‘opt-in’ service and there is a fee for the screening test. Please contact the department for further information.
Diagnosis of Chromosomal and Genetic Conditions
Chorionic villus sampling (CVS) is a test where a small sample of tissue is taken from your baby’s placenta, which is tested for chromosomal or genetic abnormalities. The test is performed between 10 weeks + 5 days and 14 weeks gestation. Amniocentesis involves taking a small amount of amniotic fluid from the pregnancy sac around the baby in the womb, which is tested for chromosomal or genetic abnormalities. This test is performed after 16 weeks of pregnancy.
Fetal Cardiology
If you have a family history of certain heart conditions or if your baby is suspected of having a heart problem on ultrasound scan you will need to attend the clinic for a fetal cardiac echo (scan) with a fetal medicine consultant. You may be referred to a special cardiac clinic in the Coombe hospital where you will meet a paediatric cardiologist. If there is an abnormality they will support and counsel you and will discuss the plan of care which is best for you and your baby.
Monitoring Fetal Growth and Wellbeing
Sometimes babies do not grow at the appropriate rate for their gestation. If this happens we will need to investigate the cause and monitor your baby more frequently with ultrasound scans during the remainder of your pregnancy.
Complicated Multiple Pregnancies
If you have a twin or triplet pregnancy you will attend a special clinic to monitor your babies’ growth and wellbeing. Sometimes babies share amniotic fluid sacs and placentas, which makes the pregnancy more complicated. However there are some treatments available if complications develop, including laser ablation.
Intrauterine Therapies
Some babies require treatment while they are still in the womb. These may include intrauterine transfusion, laser ablation, vesicocentesis and cordocentesis. We will provide you with information on any treatments you may require.
PLEASE NOTE
We will need to know your blood group if you are having any invasive procedure. Therefore, if you are not attending the Rotunda for antenatal care please bring details of your blood group with you. If you are on any medications, please contact us a couple of days before your appointment as you may need to stop or reduce your medication before the procedure.
How we will support you if there is an abnormality or problem identified with your baby
While most women give birth to healthy babies, about 3% will have a major birth defect. Most of these result from either a genetic or chromosomal disorder. When this happens we will provide parents with expert personal counselling and support and detailed information so that they can be involved in making decisions about their care. We will support you no matter what decisions you make about your pregnancy.
All the doctors and midwife specialists who work in the fetal medicine centre have had special training in diagnosing abnormalities and in supporting couples who are attending the clinic. They work very closely with the paediatric team, specialist consultants in the paediatric hospitals and with the bereavement support team, where appropriate. Weekly multidisciplinary team meetings are held to discuss patients and assist with planning the management and care for the pregnancy and birth. We will provide you with the contact details and information on the relevant support groups and organisations.
Please see the following websites for information on some genetic or chromosomal conditions:
Down’s Syndrome
Support Organisation for Trisomy 13/18
If we know that a baby may be stillborn or may not live for long after birth, parents may also wish to contact a bereavement support organisation when the diagnosis has been made. They provide helpful and important information to help and support parents at the time they are told the sad news that their baby has died or is expected to die shortly after birth.
Please see the following websites for information on these bereavement support groups and to view their information booklets.
A Little Lifetime Foundation – www.alittlelifetime.ie
Anam Cara – www.anamcara.ie
Féileacáin – www.feileacain.ie
Glucose Tolerance Test (Romanian)
Glucose Tolerance Test (Romane)
If your due date arrives and you have not gone into labour, your pregnancy is now termed ‘post mature’ or simply, overdue. Nearly half of all pregnant women are still pregnant at 40 weeks but most will go into labour in the coming week. You will be seen again in the antenatal clinic at 41 weeks if you still haven’t gone into labour. The doctor will discuss your care plan with you.
If by any chance you can’t make it to an antenatal appointment, please telephone your clinic so that another appointment can be scheduled. Towards the end of the pregnancy, your appointments will be more frequent. In the last few weeks, your GP, midwife or hospital doctor will probably see you on a weekly basis.
The medical social work (MSW) team provides a confidential support and counselling service to all women and families attending the hospital for maternity, gynaecology and paediatric care.
They can help you to access practical supports and they have up-to-date information on parent support groups, community services and welfare entitlements and benefits.
The MSW team provides counselling support and advice on issues or problems in pregnancy which can affect your wellbeing including:
The service is confidential and free of charge to all women.
Medical or midwifery staff and other healthcare staff can refer you to the medical social worker.
You can also call into the department on the day you are having an antenatal visit or phone 01 817 1722 for an appointment.
Benefits and entitlements:
Department of Social Protection
Domestic violence:
Housing:
Dublin Regional Homeless Executive
Migrants Rights: